Dr. Kishore Breaks the Back of Fake News Addiction (16)
The world has more fully awakened to the reality of fake news, of various agenda-driven media outlets hijacking narratives and exploiting the misplaced faith of their readers and viewers.

- Martin G. Selbrede
“For truth is fallen in the street…. Yea, truth faileth; … and the LORD saw it, and it displeased him that there was no judgment. And he saw that there was no man, and wondered that there was no intercessor…” [taken from Isaiah 59:14-16]
The prior fifteen articles in this series (on how Massachusetts destroyed the best drug addiction treatment developed) have gone on to become required reading in at least one college ethics course.1 We’ve reported on the documentary movie about addiction pioneer Dr. Punyamurtula S. Kishore that’s under development. In the meantime, however, the world has more fully awakened to the reality of fake news, of various agenda-driven media outlets hijacking narratives and exploiting the misplaced faith of their readers and viewers.
Two noted observers from opposite ideological poles have put their finger on what motivates such conduct on the part of the media:
Fake news is as old as the news itself. Political reporting, in particular, has always served as a tool of those who hold or seek to gain a grip on power. Respectable news sources, such as the New York Times and the Washington Post, are not and never have been strangers to the distribution of false, twisted, or selectively partial and slanted reports.2
One of the great benefits of new media—of online reporting—is that one can provide proof of one’s claims in the form of links (as I’ve done here), so that readers can determine if journalistic claims have evidentiary support. That is such a vital exercise because, as Lemann and the NYT just demonstrated, it is so often the case that the most influential media outlets publish factually false statements using the most authoritative tones.3
These dual aspects of fake news (as a tool of those who hold or seek to gain a grip on power, and publishing factually false statements using the most authoritative tones) require strong medicine to combat. We’ve been inundated with a continuing barrage of fake news concerning our nation’s addiction crisis and how it should be treated for years. Instead of moving toward Dr. Kishore’s evidence-based Massachusetts Model, the establishment is doubling down on its failed narratives with ever-greater force and frequency, worsening the spiraling death statistics. Nobody has called the media on it.
Until now.
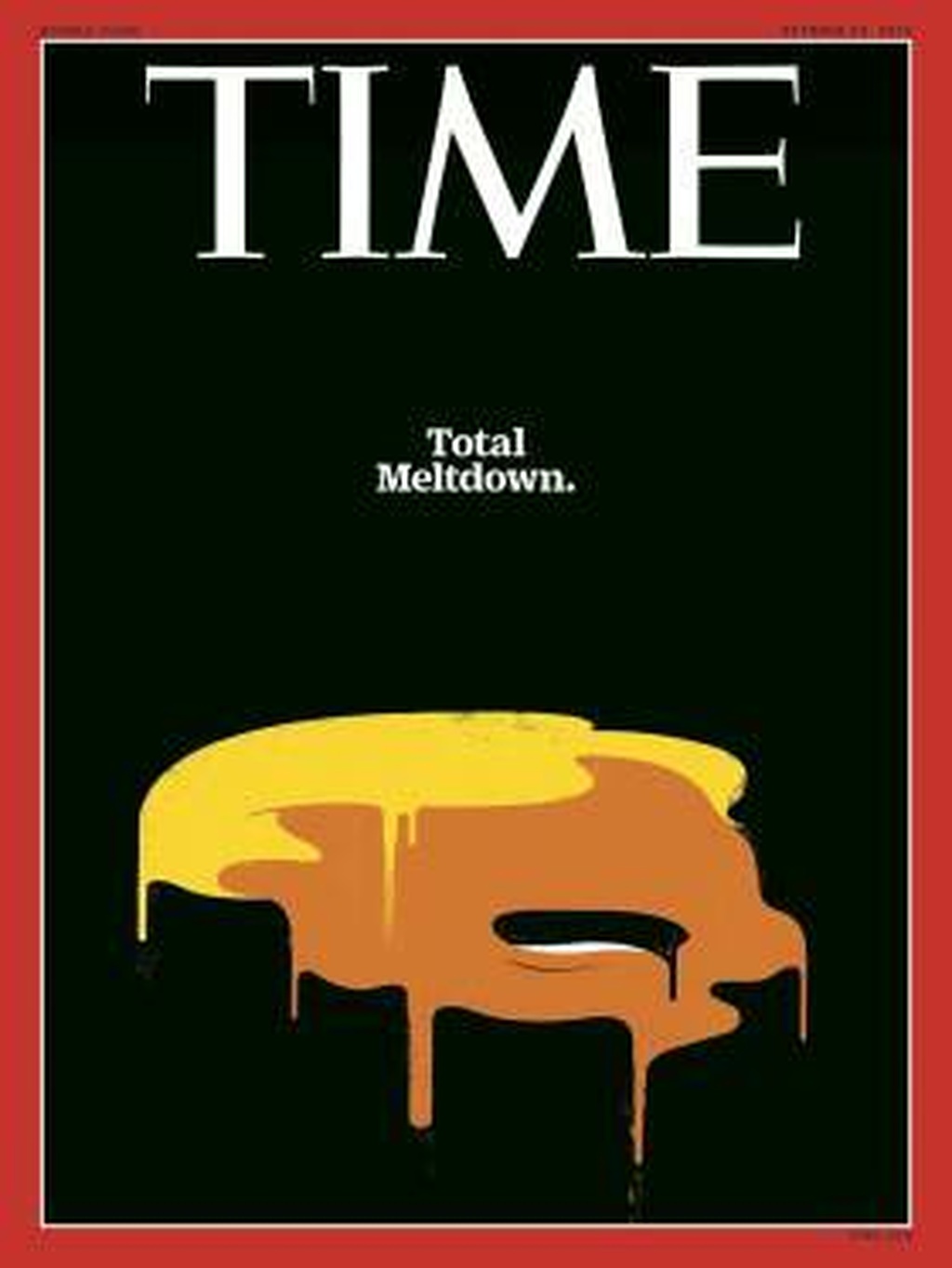
Dr. Kishore Confronts Time Magazine
Time journalist Alice Park’s article, “A new paradigm for opioid addiction: more drugs,” appeared in October of 2016.4 The embedded photo essay ups the emotional ante of the article by pushing the reader’s buttons, all carefully orchestrated to guide us to draw the same policy conclusions that Park advocates. An artfully positioned squib by the U.S. Surgeon General creates the impression of endorsement of Park’s views.
At my request, Dr. Kishore has deconstructed this Time article, walking us through its pertinent points to see the faulty reasoning driving it, and how completely it leverages reader ignorance. As such, the following “interaction” with the Time article involves heavy quotation, but Dr. Kishore’s analysis elevates the resulting narrative to the level of a “transformative work” so as not to run afoul of copyright law.
The value of this exercise will become evident upon careful reading as this hitherto unchallenged news article is given the third degree. (A similar deconstruction of a Washington Post article from January 2017 immediately follows, in which Dr. Kishore goes toe to toe against the M.D. who wrote it.)
Article quotations below appear in bold type with paraphrases in [brackets] and article descriptors in bold italics. Dr. Kishore’s responses follow in normal italics.
Dr. Kishore Cross-Examines Time’s Alice Park
Article’s title: A New Paradigm for Opioid Addiction: More Drugs
Not new at all. MAT (Medically-Assisted Treatment) has been around since 1962, without showing any outcomes.5
Photos of people passed out in cars, grocery stores, outdoors
Opioid addicts have been portrayed as recumbent since times immemorial. Nothing new. They did it in opium dens, now they do it in cars, etc. Maybe bring back opium dens or Suboxone dens or methadone dens: at least in olden times they slept safely as seen in historic photos.
“Some nights the entire shift is tied up with just overdoses,” says the police chief, John Lane.
Wrong professionals for the wrong trade: police should police while public health officials should treat. The $1.1 billion should go to enhance and beef up the United States Public Health Service Commissioned Corps6 who are sworn to “Protecting, promoting, and advancing the health and safety of the Nation.”
“We just don’t have enough people to be dealing with this problem”
Not the job of the police, despite what drug czar Michael Botticelli says.
More people died of drug overdoses in 2014...
It’s sheer stupidity (or laziness) to quote 2014 statistics when we have statistics for 2015 as well as the three quarters of 2016.
60% [due to] pain killers ... overprescription of pain killers
Meaningless numbers. Is it Oxycontin, Vicodin, fentanyl? Need specificity: vague generalities make no sense to the discerning reader.
Over the past 17 years, rates of opioid-overdose deaths have quadrupled
Then assign culpability. Last eight years it happened under Botticelli/Obama. Buck stops with the leadership. In private sector if the number went up eight years in a row the Board of Directors would fire the CEO.
... proliferation of cheaper forms of heroin and synthetic opioids
This is an illicit industry. The point indicates the reporter is foolish or uninformed. She is treating it as a legitimate business.
... depths to which opioid epidemic has penetrated U.S. communities
Obviously someone is sleeping at the wheel.
... a difficult debate over what created the problem
The answer is very simple: look at the public health triad (Agent, Host, Environment). Obama and Botticelli were allowing the Agent (drugs) to flood the country. The environment is permissive with many drugs available in the drug bazaars. The host is using and getting sick and dying. The way out of the problem is to stop the flood of drugs while improving the environment and assisting the host. It is not a difficult debate at all.
... and what’s making it worse.
No need for fear-mongering, just concerted practical action (not speeches, summits, or community forums).
Policymakers are increasingly siding with the doctors.
This is inadequate because policymakers aren’t taking guidance from doctors who are competent at producing good results.
... to rescue people with addiction from the overwhelming cravings of their habit
What a sad word, “rescue.” The Massachusetts Model produced results: patients got sober and stayed connected to their primary care providers. If you think we’re on the Titanic and need rescue boats for those in the swim, good luck. That’s not the case where it comes to addiction treatment.
Suboxone mimics ... opiates without the “addictive high”
So what? The emphasis should be on “mimics opiates.” The presence or absence of “addictive highs” is a poor benchmark or barometer when considering “addiction potential.”
Chief Lane: “We have people here abusing methadone and suboxone.”
There you go. The police chief just supported my prior statement.
“They just trade one drug for another.”
Of course they do: that is the nature of addiction.
Such concerns have led to restrictive policies governing which physicians can prescribe suboxone...
You’ve made police into doctors and doctors into police (by making them mandated vaccinators). By that logic, mandating doctors to treat addiction is next (because medicine by mandate and not by choice and mutual agreement is the lasting legacy of ObamaCare).
...and how many patients they can treat at any one time
Make the sky the limit. Obama/Botticelli do it all by executive fiat anyway.
2 million [abusers]
What is the source for her numbers? Botticelli says we have an “epidemic.”7 Epidemic means at least 7.7% of the population is infected. For the U.S., “epidemic” entails nearly 26 million addicts. Her numbers are nonsense.
Addicts ... turn to the black market
A black market is an illegal traffic or trade in officially controlled or scarce commodities. Because of porous borders the so-called commodity is not scarce. Further, we spend $31 billion8 in treatment annually (and if we use Ms. Park’s two million addicts statistic, that computes to $15,500/year per addict paid by the taxpayer). Where then is the black market opportunity and for whom?
dangerous counterfeit opioids
The fentanyl and carfentanil are coming from China9 in container ships as precursors. They are downloaded at our ports and transported to the buyers, who from what it appears are legitimately10 ordering the precursors (prodrugs) from China.11 Ms. Park is woefully inadequate in her research.12
... a bold $1.1. billion proposal
Bold? We are already spending $31 billion dollars! Without controlling drugs flowing into the country, no amount of money will solve the problem. Remember the Public Health Triad (Agent–Host–Environment). If you don’t control the mosquito you cannot control malaria.
... encourage medicine like suboxone to treat people with addictions
None of the terms are properly defined, rendering this a pseudo-sentence with indeterminate meaning.
... and allow nurse practitioners and physician assistants, as well as doctors, to receive the proper training to prescribe the drug.
What is the current curriculum? Do you have a particular curriculum you recommend? How do you measure deficiencies? What article or monograph are you citing? Your article states that doctors need only eight hours of classroom education to be certified to prescribe Suboxone. Are you recommending other measures?
[Switzerland and England] ... dispense “small” amounts of heroin
Look at the UK-Switzerland13 and USA-Switzerland14 comparisons. You’re comparing apples and oranges.
“We tend to look at addiction treatment in a black and white way,” says Dr. Joji Suzuki
How should it be looked at?
... director of addiction psychiatry at Brigham and Women’s Hospital
It’s politically incorrect to call it addiction psychiatry: Mr. Botticelli has eliminated “addiction” as a stigma word. He’d insist you rewrite Suzuki’s title as “substance user15 psychiatrist.” This PC rewrite equates three categories: the lawful doctor, the patient taking medication, and the drug pusher.
“These drug-based treatments are effective”
But Dr. Suzuki’s publications16 all pertain to his inpatient work. He followed nobody long-term. On what basis can he state that the “drug-based treatments are effective”?
“... but overall the medical culture has not embraced them.”
I have not seen any of Dr. Suzuki’s papers on “medical culture” and the “reasons” for not “embracing” “drug-based treatments.” In their absence, he has no right to make general claims, let alone pontificate.
The key is to think [of this in terms] similar to the way people take statins to lower cholesterol or insulin to keep their blood sugar in check.
Please review the statin paper17 and my comments on the diabetes analogy below. If Dr. Suzuki as a psychiatrist in the narrow field of “substance use” cannot opine on statins, surely Alice Park is even less qualified to do so.
People with addiction may be dependent on the drugs to keep them clean
Ms. Park is being politically incorrect by using the word “clean” as opposed to, I guess, being “dirty.” Both words were banished by drug czar Botticelli.
... addiction as defined in the psychiatric manual
The “psychiatric manual” Ms. Park is referring to is called DSM-5. For comparison, see Botticelli’s SAMHSA definition.18
“People tend to confuse the difference between dependence and addiction,” says Suzuki.
These are old terms no longer in use, Dr. Suzuki.
[N.b. I’ve omitted Dr. Kishore’s technical analysis of physiological dependence versus addiction due to its length. It discussed how multiple neurotransmitters contribute to reward and addiction.]
Study after study supports the effectiveness of drug-based therapies for opioid addiction.
Ms. Park completely omits opposing views19 that challenge20 this assertion.
People who take methadone and suboxone are better able to keep a job,
These are industry-sponsored studies21 if any. Comparing apples and oranges. Britain22 has socialized medicine while the U.S. does not.
... avoid relapses
Too loose a term. We need frequency of relapse, etc.23
... and gradually reduce their need to continue using heroin or opioids.
Literature advocates for gradual taper, but the “system” does not allow enough time to do a 10% of the dose every other day taper.24
That’s key to recovery...
Recovery is a loaded word that’s often ill defined.25
... opioids can have a lasting effect on the brain
Hence “recovery” is a vague, loaded word.
... rewiring reward circuits and permanently altering the way people perceive satisfaction.
Even neuroscientists find it difficult to explain the simpler case of stimulants and there’s no comparable article on opioids in the medical literature. Park’s certainty is wholly unjustified.
“Once the brain is changed by addiction, that mechanism of choice is damaged,”
Addiction to what? Opiates? Stimulants? Sex and pornography?27
What do you mean by mechanism, choice, or damage? Is this damage reversible?
... says Dr. Sarah Wakefield
I could not find a Sarah Wakefield mentioned by Ms. Park on the Massachusetts General Hospital Staff. There is a Sarah Wakeman28 who seems to have done some work with the addicted, but she is not ASAM certified, ABAM certified, or a Fellow or Distinguished Fellow of ASAM. She is just a primary care physician whose addiction work focused on policy.
... medical director of the substance-use-disorder-initiative at Massachusetts General Hospital.
Dr. Wakeman (not Wakefield) is listed as the medical director of the Substance Use Disorder Initiative and the Addiction Consult Team at Massachusetts General Hospital (MGH),29 an inpatient program. Consequently, there’s doubt she has competence in the long term care of the addicted individuals.
“It’s almost like a stroke in that part of the brain.”
The only pertinent article I can find is about smokers,30 not those addicted to opioids, which affect very different areas of the brain. These facile comparisons are not backed up by any data.
“Someone with addiction can no sooner choose not to be addicted...”
There is nothing in the medical literature to back up this contention. My practice experience directly contradicts this claim. I called addiction a “Happy Disease”31 because of the number of people I have seen in my PMAI clinics who lead healthy wholesome lives.
“... than someone with diabetes can choose not to have diabetes.”
This comparison is completely incoherent. In diabetes, the diabetics crave sugar. We are not feeding them sugar cubes every few hours like medicine: we are giving them insulin to block the cravings, and we reduce their cravings further through lifestyle modifications. Sarah Wakeman is, in effect, advocating addicts to be given “sugar cube” equivalents of methadone and Suboxone instead of blocking their cravings with Naltrexone! Her analogy does not hold water.
There remains considerable stigma
Park veers off into the bushes again with the stigma business. In contrast, look at what I did in 2008, explaining why addiction is a “happy disease” to The Woburn Advocate32 in an article that got the maximum number of clicks for a long time.
... around using drugs to treat addiction
Drugs are but tools, just as guns are. The fault lies with the people behind the guns, not with inanimate objects. Similarly, drugs are tools to get an addicted person to a sober state and into a sustained recovery process.
People with addiction who are recovering with the help of medications like suboxone are stigmatized by members of popular rehab groups ...
For addicts who wish to stay sober there is Narcotics Anonymous.33 For those who wish to stay on methadone there is Methadone Anonymous.34 For those who wish to be on Suboxone or any other drugs there is MARA.35 What are you grumbling about?
...like Narcotics Anonymous
These are “fellowship programs”36 and this is a free world where people can associate freely.37 Don’t grumble: start a group you like and ask Mr. Botticelli (who is sitting on $31 billion) to support you. Let people do what they think helps them. Why do you have to coerce Narcotics Anonymous groups to take your Suboxone Takers when there are other groups where they can go?
... discouraging them from taking advantage of the social support that’s so critical...
Nobody is objecting to you or anybody starting a Suboxone user’s group. Stop driving square pegs into round holes.
Even the good intentions of the doctors are stymied by such old-fashioned resistance.
Okay, then ask the doctors with good intentions to start a Suboxone Anonymous. After all, a doctor started Alcoholics Anonymous.38 Ask Dr. Wakeman not to sit idle but start a Suboxone Anonymous Group just as Dr. Robert Smith did in 1935 with Alcoholics Anonymous.
... physicians are restricted in how many patients they can treat with suboxone
Who is your message for? Botticelli already raised the number of patients a doctor can see from 30 to 10039 to 275. What’s the problem?
... in 2016 USDHHS expanded the number to 275 and allowed nurse practitioners and physician assistants to prescribe the drug as well.
So what is your gripe now?
Still, many doctors don’t prescribe suboxone.
Did you ask the doctors why? Might there be a reason?
... 90% of the prescriptions for it are written by just 6,000 of the 32,000 doctors in U.S. certified ...
What a revelation. Despite what you’re trying to imply, these are not heartless doctors. They see Suboxone as an inadequate way to help their patients, meaning that most doctors who practice sound medicine see no value in this drug, Ms. Park.
The certification, issued by the [DEA], involves eight hours of training on both medical and legal issues...
Make it 4 hours! Make it 1 hour! Who cares? Give it to 10% of the Workforce40 like France did41 when Suboxone was introduced there in 1992.
... no medication alone can be the answer to this epidemic.
So what is the moral of the story? If you’re shilling for more Suboxone to be prescribed, come straight out and say so, and ask Botticelli to start public clinics (as was done when methadone was first introduced here in the 1970s).
... increase options available to people with addiction
What else do you suggest besides Suboxone?
... reduce the stigma of looking for help.
Who, precisely, should reduce this “disease” of “stigma”? Aren’t psychological triggers something that puts the patient into proximity of non-stigmatizing professional doctors?
The boy [is living in] his third home in his 4 years.
Start opium dens42 like in the past so when “users” become recumbent they can be watched over by a caregiver.43 They can have babysitter services while they get high without stigma, as BHCHHP44 does. Start orphanages. [N.b. There is obvious sarcasm in Dr. Kishore’s replies here and elsewhere, provoked by the way politicized medicine has painted itself into a corner.]
.... mother ... was also a drug user
So what? Addiction is a young adult disease. It has no genetic link, meaning males and females are at equal risk. However, females tend to get pregnant. Better account for this factor when you design a service for the “user.”
mother ... left him when he was 8 days old,
What do you suggest the Mom should do? Please advise.
... his great-grandparents were awarded custody
The child was hopefully screened for this placement.
[boy was then given to] his grandmother
Okay, it is a screening issue if the grandmother is a “user” too.
... grandmother [now] serving 180 days in jail
She is a “user” under Botticelli definition, not an addict, and should not be jailed.
... her partner is serving 360 days for child endangerment
Ask Botticelli to unmess this mess.
public intoxication
If private intoxication is preferable to public intoxication, please set up a “safe site.”
driving under the influence
That is a public hazard. Because they are “users” under your preferred definition, Botticelli and cohort have to set a safe level, just like with alcohol.
While incarcerated, neither will receive treatment for drug abuse;
Why so? Did you check with the Sheriff?
... cities like East Liverpool don’t have the resources...
Why so? Can you ask Mr. Botticelli to loosen a million dollars for East Liverpool from his $31 billion?
... or the training to provide it.
Training is only 8 hours. Ask Mr. Botticelli to either shorten training to 30 to 60 minutes and offer it on the internet, or mandate all doctors to give out Suboxone.
“When they get out, they will probably go right back to what they were doing, is my guess,” says [Police Chief] Lane.
If you think they are not going to get treatment when they get out, ask your news magazine to advocate. And if you can forecast the future, and it’s this bleak, you should advocate as well given your authority in the community.
[Photo caption] A homeless addict trying to get clean in East Liverpool, Ohio, says her addiction has exhausted the patience and resources of family and friends who tried to help
Have a heart, Ms. Park. Please mobilize the community. Don’t denigrate the community where people are living. When you use the wrong tools for the wrong trade, things go horribly wrong. Good luck with this PR piece for Suboxone, Ms. Park. East Liverpool will need it, given the faulty direction you’re charting from your journalistic pulpit.
***************************************
On January 14, 2017, The Washington Post posted an article entitled “I’m a doctor who wants to treat addiction, but the rules won’t let me” by Douglas Jacobs. This remarkable story is in desperate need of cross-examination by Dr. Kishore, who had to slog through writing “of unbelievably poor quality for an MD” to measure it against the truths it hid through misdirection. At least by interacting with the article, we arrive at a “transformative work” that could actually inform the readers as to what’s truly going on. The same font style cues apply here as with Dr. Kishore’s dissection of the Time article above. Dr. Kishore has moved the penultimate paragraph to the top to better frame the issues and enhance overall clarity.
Herein lies our nonsensical system:
Can you call this a system?
We
Whom are you referring to? Speak for yourself. Use the word “I.”
physicians have
David A. Fiellin M.D.45 with his partner Dr. O’Connor at Yale University (a premier research center) set up the “system” in 2000-2001. Address your concerns in an open letter to the doctors at Yale who set up the “system” you’ve characterized as “nonsensical.”
little trouble prescribing opioids
Not so fast. Prescribing opiates comes with many checks and balances:46 DEA number, written prescription, limits on amounts, audits by DEA, Board of Medicine regulations, etc.
the very drugs
Not so fast.47 Opiates are not the only answer for pain. There are many modalities.48 Paracelsus observed, “All substances are poisons, there is none which is not a poison. It is the dose that differentiates a poison from a remedy.” Consequently, the difference between medicine, drug, and poison must be properly recognized.49
that
Drugs do not fly into people and get them addicted like a mosquito infects a person with malaria. The Drug, Set, and the Setting contribute to Addiction + Choice.
get people
Don’t call patients people. Patients are under the care of a doctor. People can do what they want. There is a major difference. Patients are under a trusted caregiver with knowledge. People, of course, are exercising free will.
addicted.
General consensus is 8% to 12% get addicted while 88% to 92% use appropriately. It is the doctor’s call to divine the risk factors.
But despite
There is no correlation. You’ve just compared apples to oranges.
an epidemic
Which “epidemic”? There are multiple “epidemics” and multiple factors50 contributing to the disease state and the spread of disease.
where 91 Americans die every day of opioid use,
Please review the CDC paper51 for the multiple contributing factors.
we face arbitrary roadblocks to prescribing addiction treatment
It is not as dire as you make it. There are provisions for override52 in all regulations.
such as training sessions and caps on the number of patients who can receive lifesaving medications.
Why are they capped? There are always provisions for overrides. Is your panel of 275 patients full? [After this point, Dr. Kishore examines the article’s title and its opening paragraphs.]
I’m a doctor [start of article title]
Dr. Jacobs is a Resident Doctor or Doctor in Training. He is not licensed to treat independently until he completes his residency and gets his license.
who wants to treat addiction
I’m glad he wants to treat addiction. Dr. Jacobs has to get the necessary Board Certifications53 before he can start practicing.
but the rules won’t let me [end of article title]
“The rules won’t let you”?! They should not let you!! Dr. Douglas Jacobs, you are not licensed in Massachusetts according to the Board of Registration in Medicine Physician Profiles54 website. This is so obviously a public relations piece, replete with bottles of Suboxone on prominent display at the top!
Dr. Douglas Jacobs is a resident physician at Brigham and Women’s Hospital in Boston. Hence he has to do everything under supervision, including writing this article. I wonder if his supervisor approved this piece.
Mr. B undid his arm bandages and revealed two large, gaping wounds where he injected his heroin. He lay back in his hospital bed, looked up at the ceiling and said with a quivering voice, “I can’t inject into my veins anymore because they are all shot. I know I have a problem, Doctor. I’ve been trying to quit, but it’s so hard.”
We need more information. Is “Mr. B” homeless? Does he have a job? Is he insured? Who is his primary care physician? What treatments were tried? We need all this before we can judge the case. Dr. Jacobs does not provide enough information but wishes to wring sympathy for his “cause.”
Mr. B (I’m identifying him only by his initial to protect his privacy)
Nice that you protected his privacy. Did you seek his consent before you used his case record for this article? Consent is paramount in research.
had been using heroin for 20 years after originally being prescribed a common opioid, oxycodone, to treat his pain.
Dr. Douglas Jacobs is giving us bits and pieces of information that slant the story without giving us a full sketch or picture of the case. In medicine we call it grand rounds: there is a format one should follow so as not to bias the audience.
He, like many others
How many did you treat?
who had fallen victim
Victim?
to the opioid epidemic,
Who declared this “epidemic” and when? What was the plan devised for warding off the “epidemic”?
was trying to quit, but methadone hadn’t worked for him.
Where did he get his methadone from? Who gave it to him? Did you review the records? Did you talk to the treater who gave him methadone? Is the story true?
“It made me feel ill,” he said.
At what dose did it make him “ill”? Is it a dosing issue? Are there blood levels drawn? Is he slow to metabolize? Is it the formulary issue? What are the symptoms of his being “sick”: nausea/vomiting? Abdominal cramps? Rash? The details are needed.
I knew of a medication that would treat his addiction
Wow! What an innovative genius you are! I’m being sarcastic because Jacobs is not a licensed doctor in Massachusetts and as such (as in the military) he works under the command and control of a licensed doctor. Dr. Jacobs, please do not claim more authority than you really have.
and possibly save his life.
Just one medication and your Mr. B.’s life could be saved! Did you report your attending physician to the Board of Medicine for cruel and unusual punishment of the patient?
It has been around for years,
Many drugs are around for years. That is no credit to the medication. What is required is case matching: is this the appropriate drug? Ignoring this is akin to malpractice.
is simple to use
It has a pretty complicated sublingual and buccal absorption. Swallowing inactivates the drug. It is not that simple.
and is safer than other options.
What, precisely, are the “different” options Dr. Jacobs considered?
Sadly,
Why “Sadly”? That is Dr. Jacobs’s fate and reality till he completes residency and gets his license.
I can’t prescribe it.
So what? You work under an attending physician who can prescribe it. If the patient is suited for care by this drug (and if deemed extremely necessary), SAMHSA55 and NAABT56 maintain websites for referral to an appropriately licensed and certified physician in the area.
We need to fix this.
Who are the royal “We”? What do you mean by “fix” this?
The drug’s name is buprenorphine, which was approved by the Food and Drug Administration in 2002.
Good. You should research DATA 200057 as well as Dr. O’Connor and Dr. David A. Fiellin, two endowed professors at the famous Ivy League Medical School at Yale University who researched and launched the drug for the federal government in 2001.
Once absorbed into the blood, buprenorphine targets the same receptor as opiates, partially blocking their effect and limiting the symptoms of withdrawal.
Dr. Jacobs failed to mention that once Buprenorphine leaves the system, in six to eight hours all the withdrawal symptoms come back with double the vengeance!
Decreased respiratory drive, which can occur with other opioids and can lead to death in overdose, occurs at a very low rate58 with buprenorphine.
However, the combination with benzodiazepines is lethal, which most addicted individuals take to get to sleep!
As such, it has become the first-line treatment for opioid addiction,
Hold a minute: first line of treatment? I heard that sobriety is the first line of treatment!
but many patients like Mr. B still have trouble getting access to the drug.
There were 1,045,91059 doctors in the U.S. in 2013. You stated 3% are certified to prescribe Suboxone: that equals 31,000 physicians. In contrast, the whole nation has only 23,000 cardiologists!60 Cardiac conditions are the #1 problem for US residents! We have 610,00061 deaths from heart related conditions in the U.S., but 570,00062 deaths from addiction.63 The manpower supply is not the problem to treat addictions—it is plentiful. According to your own statistics, it is the care system that is at fault.
Unfortunately, buprenorphine has been limited by regulations
Limitations were created by Dr. Jacobs’s own physician colleagues at Yale Medical School in 2001. Please draw them into the discussion for article completion’s sake.
that significantly hinder the drug’s widespread acceptance.
There are reasons why doctors64 have reluctance with Suboxone Practice.65
Any physician who wishes to prescribe buprenorphine has to take an eight-hour online training course.66
What’s wrong with that? Is training bad for you?
Physicians don’t have to be specially certified to prescribe other medications
Now you are comparing addiction medicine with treatment of other diseases? Every specialty has multiples of training programs!
most physicians aren’t even aware that such barriers exist.
Whose fault is that? If you want to be a doctor you pass MCAT and go to medical school. Similar systems exist for all specialties and professions! You are living in the Stone Age, Dr. Jacobs.
Unsurprisingly, 97 percent of physicians67 are not certified to prescribe buprenorphine.
The 3% who are certified amounts to a whopping 31,000 doctors! Much more than the 23,000 cardiologists we have in the country!
Arbitrary rules
Those so-called “arbitrary rules” were established by Dr. O’Connor and Dr. Fiellin. Did you contact them for comment?
handcuff
Wow! A very strong word! Are you paranoid?
the few physicians who can prescribe buprenorphine
What heroes!
capping the number of patients that each certified physician can treat
What is your wish list? How many can you treat? What exactly is your idea of treatment?
In 2000, federal legislation limited the number of patients undergoing buprenorphine treatment to 30 per physician in the first year, and 100 thereafter.
In July, new legislative changes increased the cap to 275 patients.
So that is very good! The capacity is trebled plus you did not mention they brought in Nurse Practitioners and Physician Assistants68 into the fold. That is vast capacity!
this represents an improvement,
I am glad you grudgingly “acknowledge” this.
it still limits access to crucial addiction treatment …
What other “crucial addiction treatments” are you looking for? Please explain yourself.
prevents physicians from devoting their entire practice to opioid treatment
#1 You are in training. #2 You do not have a license. #3 You are working under limited license or somebody else’s license. #4 You do not have training or board certification. #5 You have years to go before you can start a practice. #6. By the time you get to practice, the addiction epidemic may be over, as we have seen with AIDS, smallpox, cholera, etc. What is your beef?
Because of these caps, some stable patients may be forced out of buprenorphine treatment prematurely
Have you seen this happen? Are the doctors you work with so callous as to force patients out to make more slots?
to make room for a new patient with a more urgent need.
Once again you cannot speculate in medicine. If you have facts and figures, provide them or retract this article. This type of writing is hazardous to the public.
Patients like Mr. B, finally able to admit that they have problems with addiction, may have nowhere to turn.
Once again, Mr. B admitted to having a problem. But as an adult he made a choice to leave. You could have used section 12 A but you obviously felt this type of restraint is not needed. So what is the beef?
Buprenorphine has been singled out for regulation
In this land we have a code of federal regulations concerning food and drugs passed by the Congress. If you have an issue you are welcome to take it up with your Congressman or Senator.
because it is the first addiction treatment that is safe enough to be prescribed at a regular doctor’s appointment.
Once again there is the issue of Drug, Set, and the Setting. Addiction has to be viewed in the lens of that particular triangle. Drug itself is only part of the equation of treatment.
The United States has always placed strict rules on addiction treatment
You want to go to Canada? Saudi Arabia is even better: they cut the hands off alcoholics. Are you serious about “strict rules”?
partly because past addiction medications such as methadone could lead to overdose or illicit sale on the black market.
Who is selling it on the black market? Your patients? Doctors? What is the point of this sentence? The police are not doing their job right?
But buprenorphine is different.
What is blinding your objectivity here?
While buprenorphine can be sold illicitly69
Are you saying there is nothing wrong with that? Ask the Department of Correction in Massachusetts: they will tell you how it comes in Bibles and is sold for $70 a pop.
physicians can switch a patient-turned-seller to methadone
This is not easy for multiple reasons: 1. patient acceptance to go back to regimentation. 2. “slots” availability, etc.
which is administered in specialized clinics to prevent such activity
The whole purpose of Suboxone is to shut the methadone clinics! Now Dr. Jacobs wants them back in the picture! The policy is incoherent.
Additionally, the risk of buprenorphine overdose is one-fourth that of methadone, as a 2009 study70 of 16,000 people in Australia demonstrated.
So you wish to condone 25% Excess Mortality?
Even if I completed all necessary training to comply with federal regulation I still wouldn’t be able to prescribe the drug.
Why?
That’s because at the primary-care clinic where I work as a physician-in-training, none of the supervising doctors are certified to prescribe buprenorphine.
Seriously? You’re casting the blame on your superiors? In the military that is called insubordination. You would be on the path to be court-martialed.
I have been told that I shouldn’t become certified
They are wise doctors!
“you don’t want to attract those patients to your practice.”
The saying is, they are acknowledging their prudence. Sorry that they do not have your cowboy Wild West spirit. At least they are acknowledging their ignorance of an area they do not specialize in: that is truly wise.
It’s true that many clinicians view patients with chronic pain and opioid addiction as some of the hardest to take care of
Is that not true in your opinion?
We often feel torn between treating real pain and prescribing opioids to feed an addiction that could end in death.
You are so confused, Dr. Jacobs.
This is frustrating because even with the best intentions
Perhaps you and Mr. Botticelli could found, promote, and join the self-help group called Blamers Anonymous.
we are caught between pain on the one hand and overdose on the other.
So talk straight, Dr. Jacobs: what is your solution?
But this is a false dichotomy.
What is the correct dichotomy?
Treating addiction with buprenorphine instead of with opioid painkillers may make these interactions less frustrating,
Please run for Congress and change the laws.
This can and should be a positive feedback loop.
Now you are totally talking through your hat, Dr. Jacobs.
If more doctors become familiar with addiction treatment,
You want to teach them? Who should teach them? Medical Schools? Addicts?
stigma will diminish and more physicians will feel comfortable prescribing buprenorphine.
You yourself are exercising your stigma by allowing a distressed addict who is probably mentally ill walk out from under your care. How good are you? It is like the pot calling the kettle black.
But to unleash the potential of well-meaning physicians in combating our nation’s opioid epidemic,71 the first step must be to remove the barriers to prescribing this medication.
That’s a gigantic leap that applies scorched earth thinking to two centuries of progress.
Mr. B was found to have a bacterial infection in his blood, an extremely dangerous condition
Obviously if he poses a danger to himself or others by his infection, you can exercise your police powers (via Section 12 A petition).
Even so, he left the hospital before he could complete a course of antibiotic treatment.
Once again, Dr. Jacobs, if you are so concerned about the health of the patient you can issue a Section 12 A for involuntary treatment or Section 35. Further, what is the regimen you put him on? Are there other factors? Legal issues? Family issues?
He left, in part, because his opioid withdrawal symptoms were too disabling for him to deal with.
Have you heard of Section 12,72 doctor? If you are concerned you can “pink paper” Mr. B. Have you heard of comfort medicines? Have you heard of Vivitrol? Have you had a successful case of getting one anyone sober? Based on your screed you fit the pattern of a bottom feeder. Never state to yourself and others that you can help your patient in a healthy way.
He probably won’t be counted among those who die of an opioid overdose.
You are pretty morbid, Dr. Jacobs: your mind constantly veers to death of your patients. Medical schools make us into a “can do” crowd, not a bunch of whiners.
But when his infection finally overtakes his body,
Why do you wish ill for your “patient”? Are you trying to guilt trip the entire nation? You said you are a doctor? I commend to you 7 Ways to Get out of Guilt Trips.73
it will be the lack of access to addiction treatment that truly is to blame.
Wait a minute: that is a gross over-generalization, Dr. Jacobs. Further, “blame” is now the exclusive prerogative of its leading distributor, drug czar Michael Botticelli, as documented in detail by Selbrede.74 Botticelli may not appreciate the usurpation.
The complicity of The Washington Post in prominently featuring this addiction “story” while bypassing ones of actual value is a more reliable bellwether of where history will eventually place the blame for today’s rising death tolls.
In the next article in this series, we hope to probe the involvement of the United Nations in this crisis. The notion that administering a sobriety-enforcing medication like Vivitrol constitutes a human rights violation (and thus should be abandoned as a treatment option) cries out for a full examination. It appears that a frontal attack on the Biblical virtue of sobriety75 is being launched from the long-standing seat of globalist power, an attack no less oppressive than the “evangelism equals genocide” formula the UN had previously endorsed.
1. Ethics and Society, taught by Michael Gendre, Ph.D., at Middlesex Community College in Bedford, Massachusetts.
2. Robert Higgs in The Beacon. Higgs further explicates the implications for national drug policy as well: “The drug war has brought tremendous infusions of money and power into the hands of its conductors, who would be crestfallen indeed if their effort had succeeded in reducing the use and trafficking they purport to be targeting. Such success would remove the foundation that supports their hold on money and power and hence would prove personally devastating to them, however, desirable it might seem to be in the abstract.” See https://www.lewrockwell.com/20...
3. Glenn Greenwald in The Intercept. See https://theintercept.com/2017/...
4. Alice Park, “A new paradigm for opioid addiction: more drugs.” Time Vol. 188, No. 16-17, 2016 double issue dated October 24, 2016, pp. 48-53.
5. https://www.ncbi.nlm.nih.gov/b...
6. https://en.wikipedia.org/wiki/...
7. http://www.slate.com/articles/...
8. http://www.drugwarfacts.org/cm...
9. https://www.statnews.com/2016/...
10. http://www.satiratribune.com/2...
11. https://www.statnews.com/2016/...
12. http://www.wsj.com/articles/th...
13. http://country-facts.findtheda...
14. http://www.nationmaster.com/co...
15. https://www.verywell.com/dsm-5...
16. http://researchfaculty.brigham...
17. https://www.lewrockwell.com/20...
18. http://www.samhsa.gov/disorder...
19. http://blog.stjosephinstitute....
20. http://www.salemnews.com/news/...
21. http://nationalpainreport.com/...
22. http://theinfluence.org/why-is...
23. http://www.merriam-webster.com...
24. https://www.ncbi.nlm.nih.gov/p...
25. https://www.ncbi.nlm.nih.gov/p...
26. https://www.ncbi.nlm.nih.gov/b...
27. http://yourbrainonporn.com/rew...
28. http://www.massgeneral.org/doc...
29. http://www.massgeneral.org/HUB...
30. https://www.sciencedaily.com/r...
31. https://kishorewickedlocalarti...
32. https://kishorewickedlocalarti...
34. http://marsmethadone.com/metha...
35. http://www.vamarp.org/@/Recove...
36. http://www.christiandrugrehab....
37. https://www.ncbi.nlm.nih.gov/p...
38. https://en.wikipedia.org/wiki/Bob_Smith_(doctor)
39. https://www.naabt.org/30_patie...
40. http://www.baltimoresun.com/ne...
41. http://www.connexionfrance.com...
42. https://upload.wikimedia.org/wikipedia/commons/8/84/French_opium_den.jpg
43. https://www.bostonglobe.com/bu...
44. https://www.bhchp.org/news/pla...
45. https://www.ncbi.nlm.nih.gov/p...
46. https://www.cdc.gov/mmwr/volum...
47. https://blogs.scientificameric...
48. http://www.med.nyu.edu/anes/pa...
49. https://www.ncbi.nlm.nih.gov/p...
50. https://www.hindawi.com/journa...
51. https://www.cdc.gov/drugoverdo...
52. https://www.illinois.gov/hfs/M...
54. http://profiles.ehs.state.ma.u...
55. https://www.samhsa.gov/medicat...
57. http://www.buppractice.com/nod...
58. https://www.justice.gov/archiv...
59. https://www.statista.com/topic...
60. https://www.medaxiom.com/clien...
61. https://www.cdc.gov/heartdisea...
62. https://teens.drugabuse.gov/na...
63. How many people die from addiction each year? 2013 data: About 570,000 people die annually in the U.S. due to drug use. That breaks down to about 440,000 from disease related to tobacco, 85,000 due to alcohol, 20,000 due to illicit (illegal) drugs, and 20,000 due to prescription drug abuse. If you want more information, check out NIDA’s site at cdc.gov.
64. http://www.pewtrusts.org/en/re...
65. https://www.thefix.com/content...
66. https://www.samhsa.gov/medicat...
67. https://www.naabt.org/tl/bupre...
68. http://www.asam.org/quality-pr...
69. http://www.nytimes.com/2013/11...
70. https://www.ncbi.nlm.nih.gov/p...
71. https://www.cdc.gov/drugoverdo...
72. https://section12a.wordpress.c...
73. https://www.psychologytoday.co...
74. http://chalcedon.edu/research/...
75. This virtue is echoed in Stoic, Greek, and Roman cultures as well.
- Martin G. Selbrede
Martin is the senior researcher for Chalcedon’s ongoing work of Christian scholarship, along with being the senior editor for Chalcedon’s publications, Arise & Build and The Chalcedon Report. He is considered a foremost expert in the thinking of R.J. Rushdoony. A sought-after speaker, Martin travels extensively and lectures on behalf of Christian Reconstruction and the Chalcedon Foundation. He is also an accomplished musician and composer.
{kind=link}